
Precision Prevention Is Replacing Preventive Medicine

Most of medicine is still treating the past. The future is forecasting physiology.
There’s a quiet flaw in modern medicine that almost no one talks about openly:
We call it “preventive care,” but we’re still mostly reacting to early disease—not preventing it.
We wait for:
-A1c to rise
-LDL to cross a threshold
-blood pressure to stay elevated
-symptoms to become obvious
Then we intervene.
That is not prevention.
That is early treatment.
And it is exactly why chronic disease keeps accelerating despite more screening, more testing, and more guidelines.
The uncomfortable truth
Most “normal labs” are not reassuring.
They are just late signals.
By the time something is abnormal on a standard panel, the physiology has usually been drifting for years.
But medicine is still structured around a binary idea:
“normal or abnormal”
Human biology doesn’t work that way.
It works in trajectories.
And trajectories are where disease actually begins.
Precision Prevention = Medical Forecasting
A better model is emerging.
Not “preventive medicine.”
Not “functional medicine.”
Not “early detection.”
But something more operational:
Precision Medical Forecasting with active intervention control
Meaning:
1. We don’t wait for disease
2. We don’t just screen for risk
3. We continuously predict physiologic direction
5. We actively correct the trajectory in real time
This is a fundamentally different operating system.
The core shift: from thresholds to trajectories
Traditional medicine asks:
“Is this value normal?”
Precision prevention asks:
“What is this value doing over time—and where is it heading?”
That single shift breaks the entire reactive model.
Because most chronic disease does not appear suddenly.
It emerges slowly through:
- metabolic drift
- hormonal compensation
- inflammatory adaptation
- mitochondrial inefficiency
- behavioral compensation loops
By the time it’s labeled as “disease,” the system has already adapted to dysfunction.
Why “normal” is often misleading
A patient can have:
- “normal” fasting glucose
- “normal” cholesterol
- “normal” TSH
- “normal” BMI
And still be:
-insulin resistant
-inflamed at a tissue level
-losing metabolic flexibility
-trending toward disease expression
The issue is not the biomarker.
It’s the loss of temporal context.
A single data point is not physiology.
It’s a snapshot of a moving system.
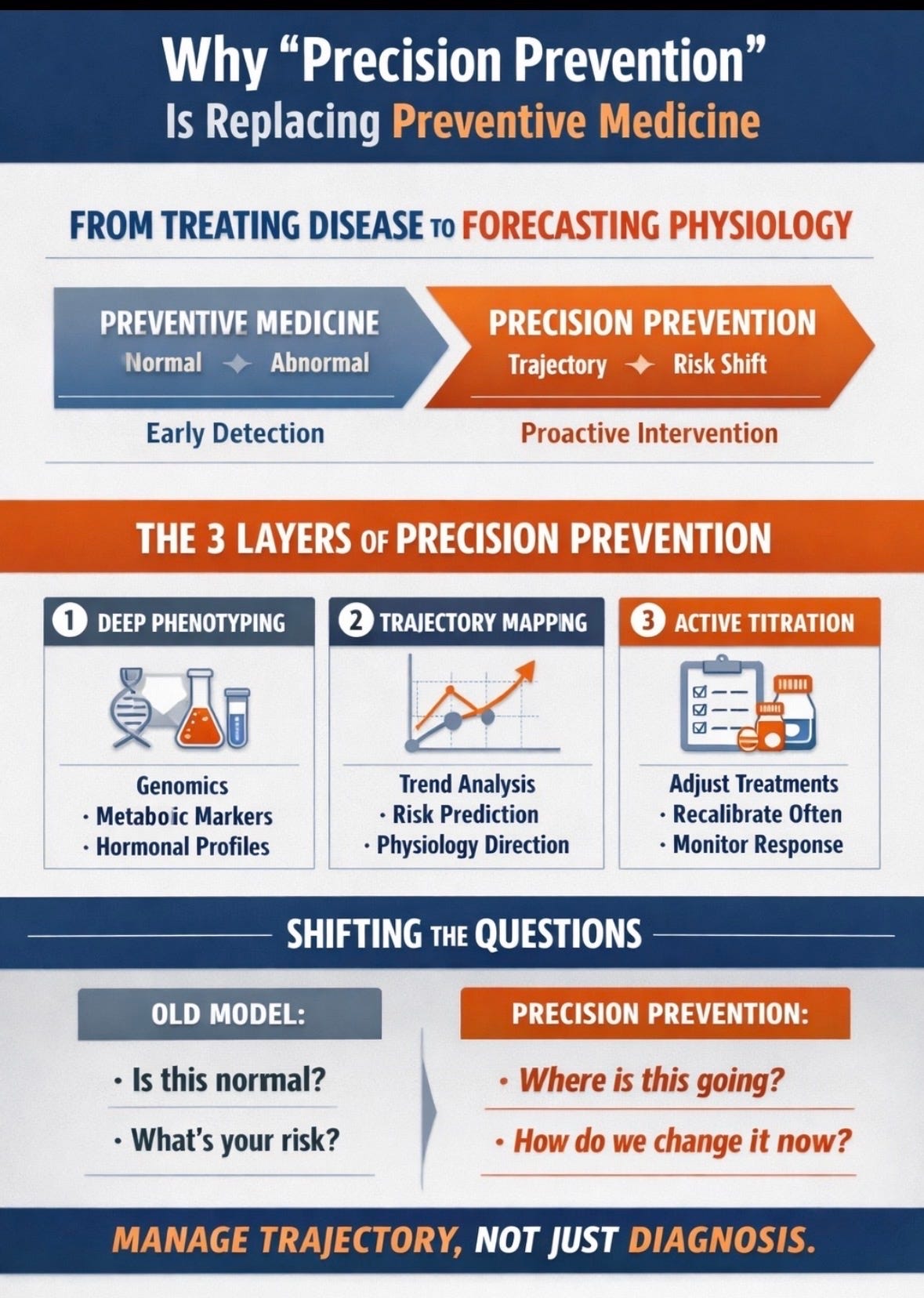
The 3-layer model of Precision Prevention
1. Deep phenotyping (what is actually happening)
This goes beyond standard screening.
It integrates:
metabolic signaling (insulin dynamics, lipid behavior)
hormonal rhythms (not just levels, but responsiveness)
inflammatory tone (baseline + change over time)
body composition shifts
behavioral physiology (sleep, recovery, stress load)
Not for information.
For pattern detection.
2. Trajectory mapping (where is this going)
This is the missing layer in most clinical care.
Instead of asking:
“Is this abnormal?”
We ask:
“Is this stable, improving, or silently worsening?”
Because the most dangerous patients are often:
“stable normals” who are actually drifting
This is where disease quietly builds momentum.
3. Active titration (changing the direction)
This is where precision prevention becomes real medicine.
Interventions are:
started earlier than guidelines would suggest
adjusted based on physiologic response
layered strategically (nutrition, movement, pharmacology, metabolic support)
continuously recalibrated
Not “prescribe and hope.”
But:
intervene → measure → adjust → repeat
A closed-loop system instead of static care.
A simple clinical reality check
Two patients have identical labs.
Conventional medicine says:
“Both are fine.”
Precision forecasting asks:
“Which one is moving toward dysfunction faster?”
Because one of them almost always is.
The difference is time—not diagnosis.
Why this matters now
We are entering a new era of medicine because three things changed:
1. We can measure physiology continuously
2. We can model patterns longitudinally
3. We can intervene earlier with more precision tools
Which means for the first time:
Disease is no longer the first signal we can act on.
It is a late signal we can often prevent.
The real disruption
Precision prevention is not about more supplements, more testing and more complexity.
It is about something simpler—and more uncomfortable:
Replacing static guidelines with dynamic decision-making.
The transition from rigid protocols to:
-more individualized trajectory assessments of aging biology
-earlier, smaller interventions
-constant recalibration
It is harder medicine.
But it is more honest physiology.
Bottom line
Preventive medicine asks:
“What should we screen for?”
Precision prevention asks:
“What is this body becoming—and how do we change that direction now?”
One reacts to risk.
The other manages trajectory.
And in chronic disease, trajectory is everything.